GLP-1s in the Real World: What 10+ Years of Prescribing Experience Uncovered (on-demand AMA webinar replay)




Key Takeaways
- GLP-1s can be powerful tools, but they aren't a standalone solution. Long-term success depends on pairing medication with nutrition and behavior change.
- Real-world outcomes often differ from clinical trials, making ongoing clinical oversight and personalized care critical to long-term success.
- Employers and health plans should evaluate GLP-1s within the context of total cost of care and implement strategies that balance access, outcomes, and sustainability.
- The most effective GLP-1 strategies offer patients multiple pathways, giving them access to medication, lifestyle interventions, and sustainable off-ramps based on their individual needs.
GLP-1s have become impossible to ignore. What was once a clinical conversation now extends into workplace benefits decisions, social media feeds, and everyday discussions about weight loss and metabolic health.

As demand for these medications has grown, employers and health plans are facing increasingly complex questions. To support the leaders navigating these continual market changes, Virta recently hosted a live Ask Me Anything (AMA) webinar featuring our clinical, member experience, and business experts. The discussion drew on over a decade of Virta’s experience prescribing, managing, and deprescribing GLP-1s and covered everything from long-term efficacy and deprescription to benefit design, cost management, and the future of GLP-1 access.
Here are the key takeaways from the discussion.
How do GLP-1s work? What are the side effects? Are they safe and effective in the long term?
GLP-1 medications mimic naturally occurring hormones that help regulate appetite, digestion, blood sugar, and insulin response. By slowing stomach emptying, GLP-1s can increase feelings of fullness, reduce appetite, and help people achieve meaningful weight loss.
Like any medication, GLP-1s carry risks and side effects. Some common side effects include:
- Nausea
- Vomiting
- Constipation
- Diarrhea
- Reflux/heartburn
- Reduced enjoyment of food due to appetite suppression
Although GLP-1s have been used in diabetes treatment for nearly two decades, there is still much to learn about the long-term impact of newer, more potent versions. Researchers continue to study the long-term effects of newer GLP-1 medications, including their impact on lean muscle mass⁷.
Many people discontinue GLP-1s within one to two years due to side effects, cost, or other barriers—and many also experience weight regain after stopping the medication².

Long-term success is more likely when GLP-1s are paired with a comprehensive care approach that includes clinical oversight, nutrition support, and long-term behavior change strategies. Because not every patient can or wants to remain on medication indefinitely, patients may benefit from access to GLP-1 off-ramps and non-medication treatment options.
What do most patients often misunderstand about GLP-1s?
- GLP-1s are powerful tools, but they don’t guarantee success alone. They were designed to be used alongside lifestyle changes like nutrition and physical activity—not as a replacement for them.
- Like any other weight loss approach, GLP-1s require behavior change. This change can be difficult to achieve and sustain without support, making coaching, clinical guidance, and structured programs important complements to medication.
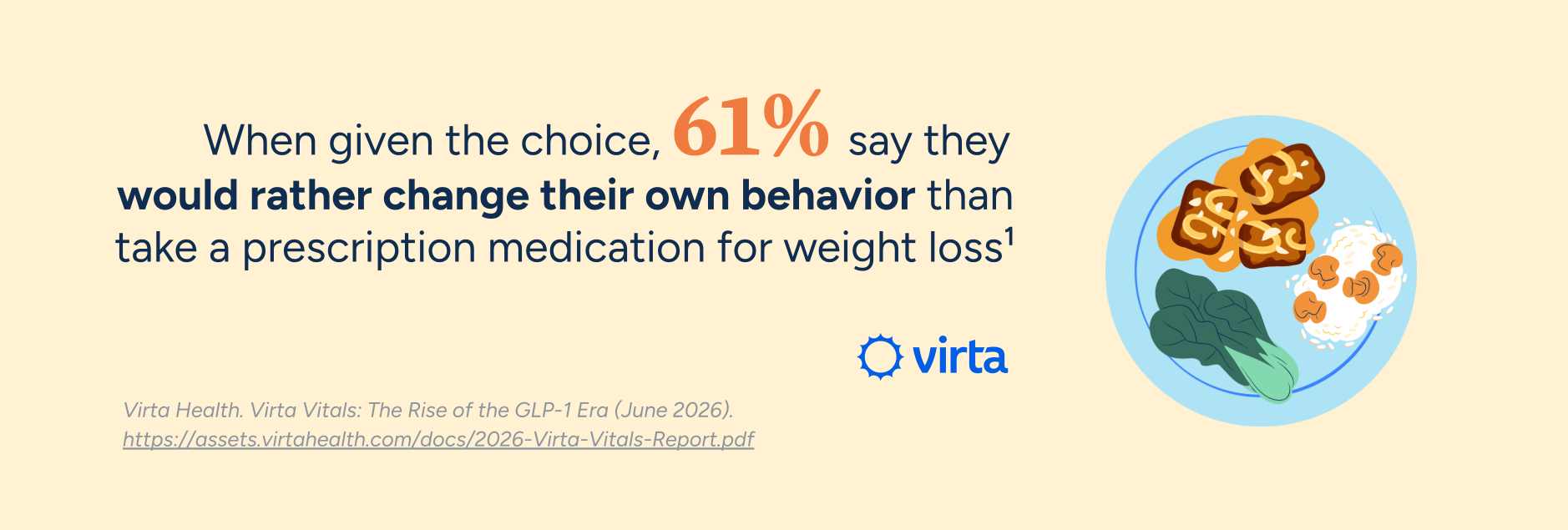
- Many patients think they want a GLP-1, when what they really want is sustainable weight loss and better health. As awareness of these medications has grown, it's easy to view them as the default solution. In reality, many people prefer non-medication approaches or a combination of medication and lifestyle support when given effective options and informed choice.
How can employers and health plans manage GLP-1 costs?
While GLP-1 prices have declined over the past several years, managing costs requires more than simply finding the lowest drug price. Employers and health plans now have multiple pathways for accessing these medications, including traditional PBM channels, direct-to-consumer programs, and emerging direct-to-employer purchasing models. The right approach depends on each organization's unique benefits strategy and population needs.
Here are a few factors to consider:
- GLP-1s should be evaluated within the context of total cost of care. Medication costs are only one piece of the equation. Employers should also consider the potential impact on related conditions, healthcare utilization, and long-term health outcomes.
- Obesity treatment costs will continue to evolve. While today's medications may be becoming more affordable, newer therapies are expected to enter the market that may offer greater efficacy⁸,⁹ but come with higher costs.
- A sustainable GLP-1 cost-management strategy should include more than medication coverage alone. Clinical guidance, lifestyle interventions, and appropriate alternatives can help patients achieve long-lasting outcomes and reduce unnecessary long-term medication spend.

How does provider support help patients achieve better outcomes with GLP-1s?
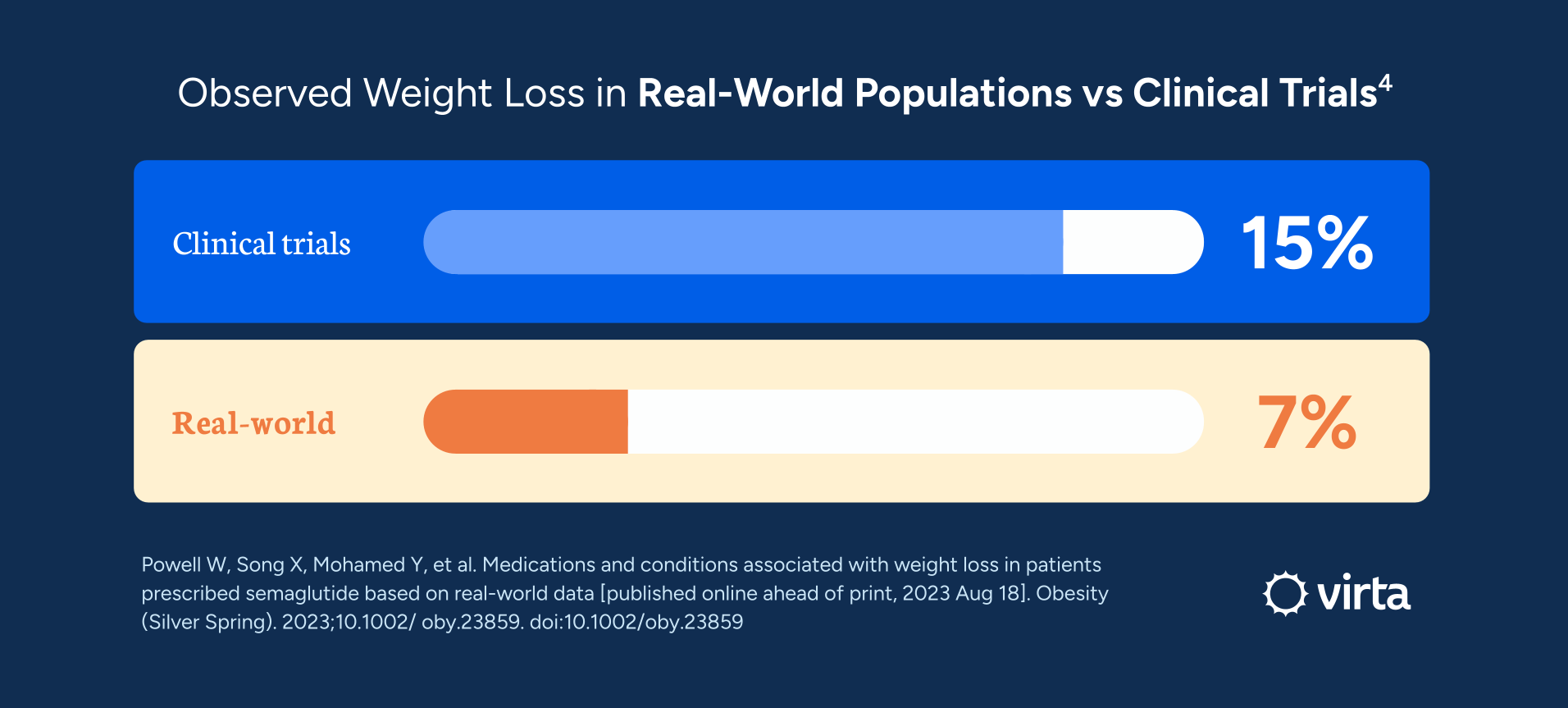
While clinical trials have demonstrated impressive weight loss outcomes, those results were achieved in environments where patients received significant behavioral support alongside the medication. In the real world, GLP-1 outcomes are often more modest.
In reality, patients struggle with side effects, take medication inconsistently, or fail to receive the nutrition and lifestyle support needed to maximize results. Experienced providers help bridge that gap with dose titration, side effect management, adherence support, and ongoing monitoring. Just as importantly, they can help patients determine whether medication, lifestyle intervention, or a combination of both is the best fit for their goals and preferences.
Ultimately, long-term success depends on more than a prescription. Building sustainable nutrition and lifestyle habits remains foundational to lasting metabolic health, whether someone chooses to take a GLP-1 or not. Provider support helps patients navigate those decisions, achieve better outcomes, and, when appropriate, successfully reduce or discontinue medication over time.
Should deprescription be part of a GLP-1 strategy? What’s it like to come off a GLP-1?
GLP-1s can be effective tools, but many patients do not want to remain on medication indefinitely. The goal is not simply to prescribe or deprescribe medication, but to help patients achieve durable metabolic health improvements that can be sustained over time.
Whether and when to stop a GLP-1 is highly individualized. Some reasons patients consider deprescription include:
- Negative side effects
- Cost and coverage challenges
- Difficulty adhering to treatment
- Reaching their health goals
- Hitting a weight-loss plateau
- Preference not to remain on medication long term
Without a comprehensive lifestyle and nutrition plan, many patients who stop GLP-1s regain the weight they lost². Building sustainable habits around nutrition, physical activity, and metabolic health can help patients maintain results long after medication is reduced or discontinued.
Virta’s GLP-1 approach is designed to support multiple paths: as a GLP-1 alternative, a co-therapy alongside GLP-1s, or using GLP-1s as a temporary tool within a broader metabolic health plan.

How are health plans managing access to GLP-1 medications?
Health plans are working to balance access with affordability and appropriate use. As demand for these medications has grown, many plans are using utilization management strategies, including:
- Prior authorization
- Step therapy
- Formulary exclusions
- Higher BMI eligibility thresholds
- Requirements for multiple obesity-related comorbidities
- Mandatory lifestyle programs
At the same time, access is becoming more complex. As new approved indications for GLP-1s continue to emerge, including uses related to cardiovascular disease and obstructive sleep apnea, more patients qualify for the medication. Off-label prescribing and alternative access channels have expanded, making it possible for some patients to obtain GLP-1s even when traditional coverage pathways are restricted.
Ultimately, many organizations are moving beyond a single ‘yes or no’ coverage decision. Instead, they’re exploring approaches that combine responsible prescribing, clinical oversight, and lifestyle support to improve outcomes while managing utilization and costs.

Are GLP-1s worth the investment for employers knowing that employees may leave before the long-term health and cost benefits are realized?
Obesity increases total medical cost by $4,800-$7,300 per person per year⁶ and carries higher risk of chronic conditions such as cardiovascular disease and diabetes, making effective treatment an important priority for employers. Many employers have high expectations that obesity treatment programs will improve health outcomes and reduce costs, yet relatively few have actually seen those benefits materialize.
GLP-1s may be a worthwhile investment, but their value depends on how they are implemented and supported. Because GLP-1s are intended to be used alongside lifestyle changes, pairing medication with nutrition, behavior change, and metabolic health support may help employers maximize the value of these medications.
Many people experience weight regain when GLP-1s are discontinued without an effective lifestyle program,² which can undermine the long-term value of the investment. Employers can improve the return on their investment by holding partners accountable for measurable outcomes and ensuring members receive the support needed to sustain results.
Watch the full AMA session for more insights
The questions didn’t stop there. During the live AMA, employers and health plan leaders also asked:
- Why is there a gap between the expectations and impact patients and plan sponsors actually see?
- Does the brand or form of GLP-1 matter when it comes to effectiveness?
- What’s going to happen with GLP-1 prices, especially with the advent of oral medications?
- If you had to design a GLP-1 benefit from scratch today for a self-funded employer, what coverage criteria and clinical guardrails would you implement first?
Watch the on-demand AMA webinar to hear how Virta's experts approach prescribing, managing, and deprescribing GLP-1s—and what employers and health plans should consider when building a sustainable strategy for the years ahead.
Related Resources
This blog is intended for informational purposes only and is not meant to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or any advice relating to your health. View full disclaimer
Are you living with type 2 diabetes, prediabetes, or unwanted weight?

- Virta Health. Virta Vitals: The Rise of the GLP-1 Era (June 2026). https://assets.virtahealth.com/docs/2026-Virta-Vitals-Report.pdf
- West S, Scragg J, Aveyard P, Oke J L, Willis L, Haffner S J P et al. Weight regain after cessation of medication for weight management: systematic review and meta-analysis BMJ 2026; 392 :e085304 doi:10.1136/bmj-2025-085304
- Prime Therapeutics. Real-World Analysis of Glucagon Like Peptide-1 (GLP-1) Agonist Obesity Treatment Year-Two Clinical and Cost Outcomes (July 2024). n=3,364. Commercial data from people with obesity or BMI ≥ 30. https://www.primetherapeutics.com/documents/d/primetherapeutics/prime-mrx-glp-1-year-two-study-abstract-final-7-10
- Powell W, Song X, Mohamed Y, et al. Medications and conditions associated with weight loss in patients prescribed semaglutide based on real-world data [published online ahead of print, 2023 Aug 18]. Obesity (Silver Spring). 2023;10.1002/ oby.23859. doi:10.1002/oby.23859
- McKenzie, A.L., Athinarayanan, S.J. Impact of Glucagon-Like Peptide 1 Agonist Deprescription in Type 2 Diabetes in a Real-World Setting: A Propensity Score Matched Cohort Study. Diabetes Ther (2024). https://doi.org/10.1007/s13300-024-01547-0
- Ward ZJ et. al. “Association of body mass index with health care expenditures in the United States by age and sex” PLoS One. 2021
- Alexandr Ceasovschih, Andreea Asaftei, Maria Giovanna Lupo, Stanislav Kotlyarov, Hana Bartušková, Anastasia Balta, Victorita Sorodoc, Laurentiu Sorodoc, Maciej Banach. Glucagon-like peptide-1 receptor agonists and muscle mass effects. Pharmacological Research. Volume 220, (2025). https://doi.org/10.1016/j.phrs.2025.107927
- W.T. Garvey, M. Blüher, C.K. Osorto Contreras, M.J. Davies, E. Winning Lehmann, K.H. Pietiläinen, et al. Coadministered cagrilintide and semaglutide in adults with overweight or obesity. New. Engl. J. Med., 393 (7) (2025). https://doi.org/10.1056/NEJMoa2502081
- Bajaj H, Welch M, Shah P et al. Efficacy and safety of retatrutide, a GIP, GLP-1, and glucagon receptor agonist, in people with type 2 diabetes and inadequate glycaemic control with diet and exercise (TRANSCEND-T2D-1): a double-blind, randomised, phase 3 trial. The Lancet, 2026; 407, 2402-2413. https://doi.org/10.1016/S0140-6736(26)00967-0