To Fast or Not to Fast: What Are the Risks of Fasting?




Key Takeaways
- Fasting beyond 24 hours has not been proven to sustain long-term weight loss, and it begins breaking down lean tissue and lowering resting metabolism.
- Fasts longer than one day can sharply change medication needs for diabetes and blood pressure, creating real risk for hypoglycemia, hyperglycemia, and other complications without close supervision.
- Prolonged fasting can also increase the risk of refeeding syndrome when eating resumes, especially after longer fasts, chronic dieting, illness, or mineral depletion.
- Virta Health focuses on a well-formulated ketogenic approach that preserves lean tissue and essential minerals while supporting weight loss and metabolic health without the instability of repeated fasting.
Fasting in various forms is getting a lot of media attention. Its advocates, with varying degrees of expertise and medical training, claim that it is an easy way to speed weight loss and get into ketosis, and that it is safe to do without medical supervision. We beg to differ. Looking at the published science, and particularly the long-term safety and efficacy of fasting, there are a number of reasons to be concerned with this approach to weight loss and metabolic health.
Defining the various forms of fasting
- Partial day fasting. Intermittently skipping one or two meals per day, resulting in no calorie intake for periods of 18 hrs (eg, no breakfast) to 24 hrs (no breakfast and lunch) on alternating days. Another version is no food during daylight, as practiced during the Muslim month of Ramadan.
- Single day fasting. No food or calories from the evening of day #1 to the morning of day #3 – a span of 36 hours.
- Multiple day fasting. No food or calories for 48 hours or longer.
- 5:2 intermittent fasting. 2 days per week restricted to 500-600 kcal per day, whether consecutive or separated by one or more days of unrestricted eating.
In brief, any regimen involving fasting beyond 24-hours has not been proven effective in sustaining weight loss long term. And while it can temporarily speed weight loss, this comes with a long-term price. After just one day of fasting, you begin to lose body protein from lean tissue – from places like muscle, heart, liver, and kidneys. These organs and their functions are things that we want to preserve, and definitely should not be given up lightly. So while you may lose weight according to the scale, part of it will be at the cost of your important, metabolically active tissue.
This is why we make the distinction between ‘nutritional ketosis’ and ‘fasting ketosis’ in our books and in our presentations. When done correctly, nutritional ketosis is achieved while maintaining lean tissue protein and function. In contrast, fasting ketosis reduces your resting metabolism, your strength, and your bodily functions.
Yes, the human body is equipped to survive fasting for days, weeks, or even a month or two. This is how we humans have evolved to survive disease or famine. But for each 24-hour period that we fast after the first day, we need 2-3 days of optimum food intake to recover what we’ve lost. So while theoretically a person could do a total fast for two days per week and still manage to get caught up in between, where is the science showing that we can recover that lean tissue and metabolic rate without overeating during those catch up days? The answer, to date, is that no one has published the research showing that this is safe to do for months at a time.
The other obvious safety concern with fasting, whether intermittent or sustained, is its effects on medication requirements to manage diabetes, heart disease, or high blood pressure, and possible anti-coagulation (aka blood thinners) as well. For people with type 2 diabetes in particular, medication requirements for adequate blood glucose control are dramatically reduced in just the first day or two of fasting or carbohydrate restriction, making close medical supervision mandatory. But then these medications need to be promptly resumed upon re-introduction of dietary carbohydrates. Doing this repeatedly in an intermittent pattern engenders significant risk of acute hypoglycemia or hyperglycemia. Similarly, blood pressure is often markedly reduced in just the first few days of fasting, requiring similar prompt medication adjustments down and then back up.
And finally, it has been known for almost a century that people rescued from starvation (e.g., a famine, lifeboat, or concentration camp) are at risk of sudden death if they are abruptly given lots of food. This has an official medical name – ‘refeeding syndrome.' The solution is controlled refeeding under expert supervision. For most people who are well-nourished before fasting (whether by choice or not), it takes at least a week or two of fasting before refeeding syndrome could pose a risk. But previous dieting, previous fasting, age and illness can shorten this interval before the risk for sudden death begins.
So where is the tipping point at which the duration of a fast becomes counter-productive?
The simple answer is: “It depends”. If you have diabetes and are taking a medication like insulin, reducing or stopping your carbohydrate intake for just one day will dramatically change your medication needs for that day. This in turn will alter how you respond to your medications when you add back dietary carbs, setting off a blood glucose roller-coaster. If you have a physically demanding job, on day #2 of fasting, you are likely to ‘hit the wall,’ resulting in a dramatic reduction in both physical and mental performance. If you already have marginal levels of important minerals like potassium and magnesium – common problems in people with diabetes or in people taking diuretic medications – how will you make up for the losses of those minerals which continue or accelerate on the days that you don’t eat?
We know that a well-formulated ketogenic diet sustains (if not improves) a person’s health and function, both during weight loss and also in weight maintenance. One key attribute of a well-formulated ketogenic diet is that it preserves lean tissue and essential minerals from day-to-day without generating deficits requiring catch up. Yes, it is true that one can lose weight more rapidly with total fasting or with very low calorie diets, but neither of these is sustainable. When looked at from the perspective of your health and function over months or years, why take the risk?
The Scientific Details
Let’s start with a few pictures from old but excellent human research. This is what fasting does to lean tissue:
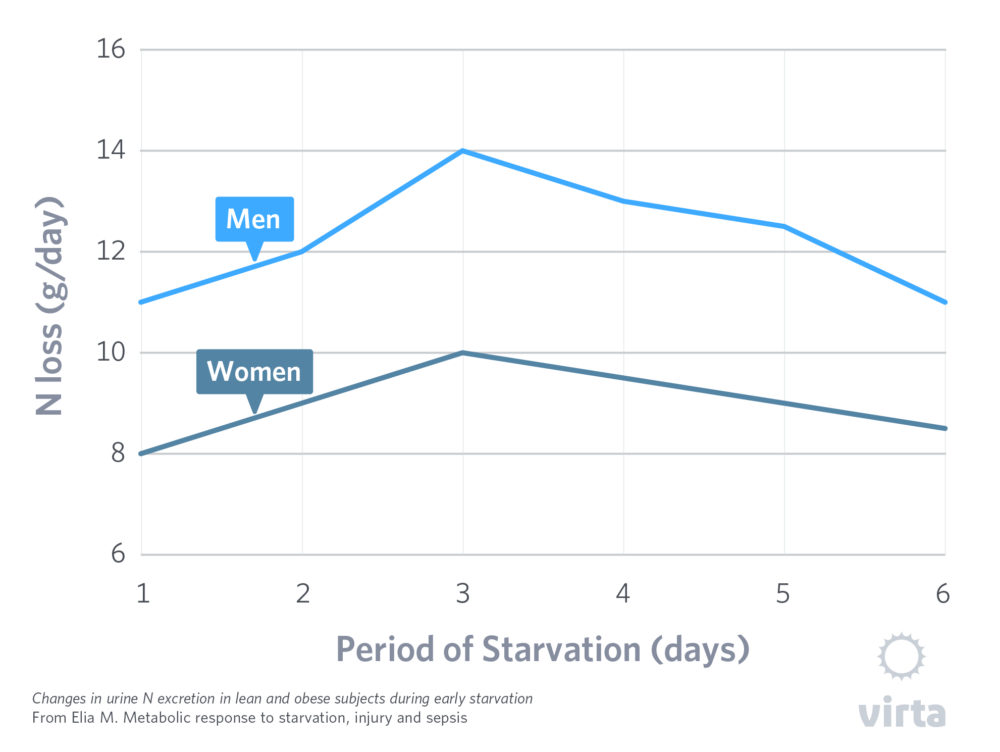
In Figure 1, nitrogen (‘N’, i.e., protein) is lost starting on day 1, reaches a maximum on day 3, and then slowly declines. The losses are shown in grams of nitrogen per day, where each gram represents the loss of about 1 ounce of lean tissue. These results have been validated in many human studies, including Owen et al, 1969.
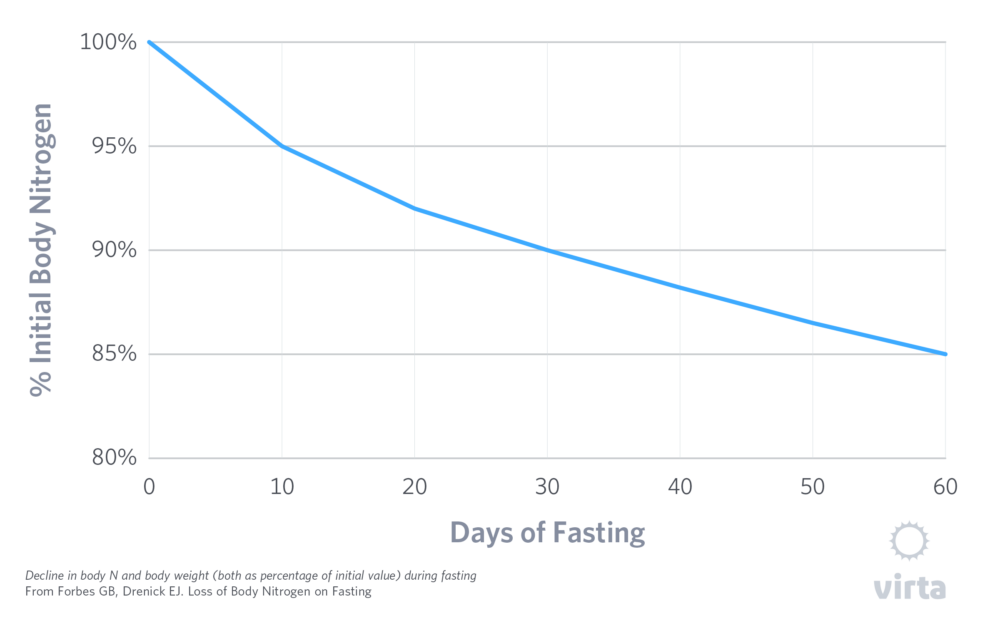
Figure 2 shows the long-term loss of body nitrogen (i.e., protein) as % of one’s pre-fasting value. Note that these losses slow slightly after the first 10 days but never stop.
Translation: healthy overweight adults on a total fast lose 5 lbs of lean tissue at 10 days and 10 lbs after 30 days.
And this is what prolonged fasting beyond 2-3 days does to resting metabolic rate (REE), which when measured in the morning before activity or food is called basal energy expenditure (BEE).
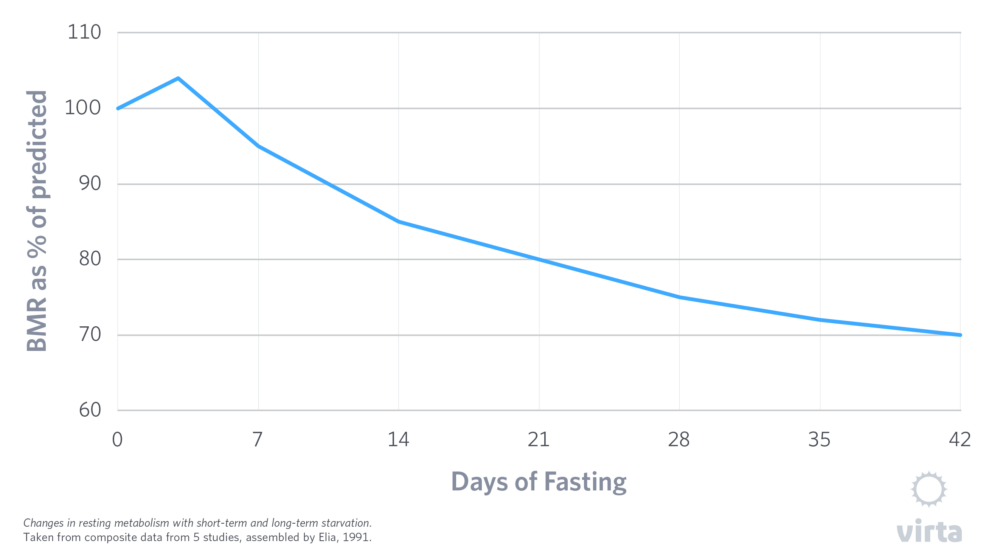
What this classic study showed was a 15% reduction in BMR (ie, resting metabolism) after 10 days of fasting and 25% reduction after 30 days. Far from being refuted with more modern research methods, these original observations have been confirmed over and over in the published medical literature.
Yes, there is evidence that there is a transient 1-3 day slight rise in REE when lean subjects begin total fasting (Webber, 1994), and this is caused by a rise in serum norepinephrine – a stress response to initiating a fast (Zauner 2000). But the REE then falls below and stays below the starting baseline after the third day. (Elia 2001; Drenick, 1973; Rabast 1981).
The Scientific Details of Fasting and Protein Metabolism
The human metabolic response to fasting has occupied a necessary role in our survival over the past few million years. An adequately nourished adult can survive for 60 days or more without food, when given adequate water and sodium. But the price of total fasting (i.e., when neither protein nor other calories consumed) is literally paid in pounds of lost flesh.
As shown above, net protein breakdown begins within the first day of fasting, reaches its maximum rate within 2-3 days – typically a pound of lean tissue lost per day – and then slowly tapers to 'just’ a quarter pound per day after 4-5 weeks. It is also well established that extra adipose tissue does little to protect the body from this pattern and rate of lean tissue catabolism. Yes, it is true that some severely obese individuals have been documented to survive fasts much longer than 60 days, but only because their extreme obesity was also associated with greater underlying lean body mass (LBM) to begin with.
It is also worth pointing out that people do not carry around ‘extra’ protein stores held in reserve doing nothing — just waiting to fill in for the day we don’t eat enough dietary protein. All protein in the human body has a real-time function, be it muscle, connective tissue, red blood cells, brain, or antibodies. So whenever the body loses protein, it loses some of its functional reserve. How much functional reserve each of us has (i.e., how much protein we can lose before it threatens survival) is quite variable. For example, some very obese people build some extra muscle to be able to carry their weight. But on average, once someone loses one-third of their initial LBM, they are functionally debilitated; and when they reach 50% of normal LBM, any further loss of protein is imminently fatal.
All of these observations were well established by studies performed between 1910 and 1980. Of particular note was the Minnesota Experiment done on imprisoned conscientious objectors during WWII (the Biology of Human Starvation, Univ MN Press, 1950) and by George Cahill’s group in the 1960’s (Owens et al, JCI, 1969). Subsequent to that, there was an active period of research on ‘supplemented fasting’ in the 1970’s, including studies demonstrating the preservation of both lean body mass and physical performance with well-formulated ketogenic diets.
Taking into account that it requires at least 4 weeks for most of the body’s adaptation to energy/carb restriction to occur, the following 4 studies provide useful information on protein intake and preservation of lean body mass, performance, and metabolic rate during nutritional ketosis and total fasting.
1. Rabast et al, 1981.
Total fasting was compared with a 300 kcal/day very low calorie diet providing 56 g protein and 12 g carbs in 14 healthy obese patients, selected as matched pairs, over a period of 28 days. The weight loss was significantly greater during fasting than during the VLCD (16.5 kg vs. 12.7 kg). The basal metabolic rate showed a significant decrease (25 per cent) during total fasting, but was unchanged with the VLCD. With both diets there was no significant change in T4 or TSH, but T3 decreased along with a transient increase in rT3. Nitrogen balance was attained in five of seven patients on the VLCD after four weeks but none of the patients on the total fast.
2. Marliss, NEJM, 1978.
Obese subjects followed three different protocols:
- A supplemented fast providing 82 grams of protein in 400 kcal per day for 21 days. Despite this level of protein intake, lean tissue losses occurred promptly and persisted for 2 weeks, after which ‘nitrogen balance’ (ie, no further loss of lean body mass) was re-established. Expressed in grams of protein per kg of reference weight, this protein intake represented 1.2 g/kg per day.
- A supplemented fast providing 82 grams of protein in 400 kcal per day for 7 days, followed by 14 days of slowly reducing protein/calories down to 41 g/d of protein in 200 kcal at day 21. As above (a), nitrogen balance was similarly negative for the first 7 days, after which the further step-wise reduction in protein caused ongoing lean tissue wasting out to 21 days. In other words, even 21 days of keto-adaptation would not allow for lean tissue preservation at the 41 g/d protein intake level.
- 21-28 days of total starvation, followed by 7 days of a supplemented fast providing 92 grams of protein in 400 kcal per day. As expected, lean tissue losses were rapid during the starvation phase (> ½ lb/day), but then flipped to ¼ lb/day of lean tissue gain when adequate protein intake was resumed. In this situation, however, it is important to note that lean body mass recovery occurred at less than half of the rate that it was lost during total fasting.
3. Phinney, JCI 1980; and Phinney Metabolism, 1983.
In these 2 studies, 6 obese, untrained subjects and 5 highly trained bicycle racers were tested for fitness and endurance at baseline, and then given 1.2 to 1.75 g of protein per kg of reference weight for 4-6 weeks of a ketogenic diet. In this range of protein intakes, there was no measurable loss of peak aerobic power (VO2max) or endurance time to exhaustion. In other words, adequate protein intake in the context of a well-formulated ketogenic diet can promptly and effectively restore normal lean tissue functions. And in the 5 bicycle racers, daily measurements of protein intake and nitrogen excretion confirmed that lean body mass was effectively maintained across the 4 weeks on the ketogenic diet at 1.75 g/d of protein intake.
4. Davis and Phinney. Int J Ob 1990.
Ten obese women were randomized to very low calorie ketogenic diets providing either 1.2 or 1.5 g protein per kg reference weight for 4 months. Weight losses averaged 17 kg. Compared to baseline, VO2max and peak quadriceps strength declined on the 1.2 g/kg protein dose, whereas both of these functions were preserved at the 1.5 g/kg level.
Intermittent Fasting
Given the current popularity of intermittent fasting (IF), one would assume that there would be well-designed studies published to demonstrate that its practice does not impair lean tissue preservation or function in humans. Unfortunately, this is not the case. Yes, there are multiple published studies of ‘intermittent fasting,’ defined as not eating from morning until early evening every other day, or not eating any protein until the evening meal. There are also a few studies of people eating 75% less or total fasting for every other day or in a 5:2 sequence. Weight losses are typically range from 2% to 5% but plateau quickly. At this amount of weight loss, accurate measurements of body composition are problematic, so good data on lean body mass changes are lacking. Nonetheless, what published data there are do not raise any major red flags for people practicing partial day fasting, even on a fairly regular schedule.
Given that people doing intermittent fasting are eating a lot less than they need a few days per week, one has to ask why do they stop losing weight so quickly? One answer can be found in a study by Heilbron et al., in which subjects doing every-other-day fasting reported increased and sustained hunger across this 22-day study.
But many people who practice ‘intermittent fasting’ eat nothing or no protein for more than one day at a time. Based upon the published science, this is where the health risks begin, even if this information is denied or glossed over by the advocates of fasting. More importantly, when people choose to fast for many days at a time, these risks rapidly escalate due to losses of protein and essential minerals. And assertions that the human body can effectively conserve its functional tissue and resting metabolic rate across many days of total fasting appear to be based upon ideology, not on solid science.
There are other reasons why people fast besides weight loss. Boosting blood ketone levels is increasingly associated with reduced aging and oxidative stress in animal studies. There are also many reports of energy restriction reducing cancer growth in animals, but this benefit is not consistently seen with intermittent fasting in animals, implying that the benefit is in consistent restriction rather than intermittent restriction. And the early data on intermittent fasting and even ketogenic diet in humans with cancer are inconsistent.
Lean Body Mass and Energy Expenditure
There is a rich literature on human recovery of lean tissue and function following energy restriction or protein deprivation. In the Minnesota Experiment during WWII, for example, lean healthy males who were fed ‘half-rations’ (1600 kcal and 50 g/d protein) for 6 months lost ⅓ of their lean body mass, leaving them functionally debilitated. Once refeeding with adequate protein and energy was begun, it took them over 4 months to approach their original baseline of strength and function, and in so doing, they added excess body fat.
In addition to the Marliss study quoted above, multiple human studies demonstrate that the maximum rate at which a protein-deprived person can gain back lost lean body mass is ¼ pound per day (ie, 4 g/d positive nitrogen balance). So if a day of total fasting causes the loss of ½ to 1 pound of lean body mass per day (depending upon one’s level of keto-adaptation), then it takes at least 2-4 days of full feeding with protein and energy to recover that one day’s lean tissue loss. And as the Minnesota Experiment and many others have shown, this recovery of lost lean tissue usually occurs along with a gain in extra body fat as well.
So what does this really mean? Yes, total fasting can cause rapid weight loss, but typically half or more of this will come from lean tissue. And most importantly, depending upon the amounts of protein and energy one consumes after a period of fasting, the rate of recovery of lean tissue will likely be slower than the rate at which it was lost. To be blunt, in the real world, recovery of lean tissue after total fasting takes a lot longer than the period of fasting itself.
And finally, there is the impact of fasting on resting metabolism. Think of your metabolism being controlled by two separate factors: (1) your ‘thermostat’ and (2) your ‘furnace.’ The amount of lean tissue you have is a strong determinant of your resting metabolic rate. Interpretation: your total muscle mass is your furnace – the more muscle you have the faster you can burn energy. But your body also has an elegantly tuned thermostat, that determines how much energy your furnace burns. And that is regulated by the combination of active thyroid hormone (T3) production and tissue thyroid hormone sensitivity.
We know from many human studies that when people are subjected to acute starvation, resting metabolism drops by about 15% in the first 10 days – ie, long before 15% of lean tissue is lost. In other words, the thermostat is turned down well before the furnace gets smaller. However when dietary carbs are limited but adequate protein provided, the ‘thermostat reduction’ (as measured by resting metabolic rate) is much less, and the size of the furnace is maintained. Thus, whereas fasting beyond the first day or two extracts a big price in metabolic energy expenditure (thermostat plus furnace), a well-formulated ketogenic lifestyle does not.
Refeeding Syndrome
This commonly fatal problem has been known since World War II, when rescued people with acute or chronic starvation suddenly developed congestive heart failure and abnormal heart rhythms when given lots of food. Given the risk of death, it has never been studied (nor should it be) with a randomized controlled trial. But it clearly involves rapid shifts of fluid and electrolytes/minerals with the movement of protein and glycogen into cells, as well as the reversal of the natriuresis of fasting. It is assumed that refeeding syndrome was the cause of death for the singer Karen Carpenter in 1983, who died after being admitted to hospital because of lean tissue wasting from anorexia nervosa. It has also been reported in numerous malnourished hospitalized patients who are refed intravenously.
The specific conditions that may lead to refeeding syndrome are not well defined, but chronic dieting and definitely periods of fasting beyond a day or two are significant concerns. Chronic illness or medications that cause mineral wasting (ie, poorly controlled diabetes or diuretic use) can be contributors as well.
The best way to deal with refeeding syndrome is to prevent it from occurring. This means consuming a diet adequate in essential minerals when dieting, and also avoiding wide swings in energy and nutrient intakes, especially at a time when one is undergoing weight loss. We also know that breaking nutritional ketosis with a lot of carbohydrate can cause dramatic fluid retention plus a shift of potassium, magnesium, and phosphorus into cells (all characteristics of refeeding syndrome). So when adding carbs to your intake, this is best done in moderation. But most importantly, why set yourself up for this problem by creating fasting-induced protein and mineral deficits in the first place?
Conclusions
- The current practice of intermittent fasting has outpaced the published human data supporting its use, particularly in weight control and promoting nutritional ketosis.
- There is the strong potential that lean tissue losses can become significant when full fasting days are more frequent that once or twice per week (and this caution may apply to resting metabolic rate as well).
- Medications for diabetes and high blood pressure require prompt and expert management when initiating a fast longer than 24 hours. Improper medication management carries significant health risks.
- Rather than pursue acute and dramatic weight loss by fasting—even if it is just ‘intermittent’—it is better to take the long-term view and avoid doing things that can compromise lean tissue and function. Health is defined by where you will be 1 year or 1 decade from now, not where you will be in 1 week or 1 month.
Dr. Phinney on fasting
Have more questions about nutritional ketosis? Check out our FAQ by Dr. Steve Phinney and the Virta team.
The information we provide at virtahealth.com and blog.virtahealth.com is not medical advice, nor is it intended to replace a consultation with a medical professional. Please inform your physician of any changes you make to your diet or lifestyle and discuss these changes with them. If you have questions or concerns about any medical conditions you may have, please contact your physician.
This blog is intended for informational purposes only and is not meant to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or any advice relating to your health. View full disclaimer
Are you living with type 2 diabetes, prediabetes, or unwanted weight?

- Davis PG, Phinney SD. Differential effects of two very low calorie diets on aerobic and anaerobic performance. Int J Obes. 1990 Sep;14(9):779-87.
- Drenick EJ, Dennin HF. Energy expenditure in fasting obese men. J Lab Clin Med. 1973: 81:421-30.
- Elia M. Metabolic response to starvation, injury and sepsis. In: Artificial Nutrition Support in Clinical Practice: Second Edition Edited by Jason Payne-James, George K. Grimble and David B. A. Silk. (2001); Cambridge University Press. 978-1-107-60965-5
- Elia M. 1991. http://archive.unu.edu/unupress/food2/UID07E/UID07E12.HTM
- Forbes GB, Drenick EJ. Loss of Body Nitrogen on Fasting. Am J Clin Nutr. (1979) 32:1570-1574.
- Goschke H, Stahl M, Tholen H. Nitrogen loss in normal and obese subjects during total fast. Klinische Wochenschrif. 1975;53:605-10.
- Halberg N, Henriksen M, Söderhamn N, Stallknecht B, Ploug T, Schjerling P, Dela F. Effect of intermittent fasting and refeeding on insulin action in healthy men. J Appl Physiology. 2005; 99: 2128-2136 DOI: 10.1152/japplphysiol.00683.200
- Heilbronn LK, Smith SR, Martin CK, Anton SD, Ravussin E. Alternate-day fasting in non-obese subjects: effects on body weight, body composition, and energy metabolism. Am J Clin Nutr. 2005; 81:69-73.
- Keys A, Brozek J, Henschel A, Michelsen O, Tayler HL. The biology of Human Starvation. Univ of MN Press. Minneapolis MN, 1950.
- Marliss EB, Murray FT, Nakhooda AF. The metabolic response to hypocaloric protein diets in obese man. J Clin Invest. 1978 Aug;62(2):468-79.
- Nair KS, Woolf PD, Welle SL, Matthews DE. Leucine, glucose, and energy metabolism after 3 days of fasting in healthy human subjects. Am J Clin Nutr. 1987; 46:557-562
- Owen OE, Felig P, Morgan AP, Wahren J, Cahill GF, Jr. Liver and Kidney Metabolism during Prolonged Starvation. J Clin Invest. 1969; 48:574-583.
- Phinney SD, Horton ES, Sims EA, Hanson JS, Danforth E Jr, LaGrange BM. Capacity for moderate exercise in obese subjects after adaptation to a hypocaloric, ketogenic diet. J Clin Invest. 1980 Nov;66(5):1152-61.
- Phinney SD, Bistrian BR, Wolfe RR, Blackburn GL. The human metabolic response to chronic ketosis without caloric restriction: physical and biochemical adaptation. Metabolism. 1983; 32(8):757-68.
- Rabast U, Hahn A, Reiners C, Ehl M. Thyroid hormone changes in obese subjects during fasting and a very-low-calorie diet. Int J Obes. 1981;5(3):305-11.
- Webber J, Macdonald IA. The cardiovascular, metabolic and hormonal changes accompanying acute starvation in men and women. Brit J Nutr. 1994; 71:437-447
- Zauner C, Schneeweiss B, Kranz A, Madl C, Ratheiser K, Kramer L, Roth E, Schneider B, Lenz K
- Resting energy expenditure in short-term starvation is increased as a result of an increase in serum norepinephrine. Am J Clin Nutr. 2000; 71:1511-5.