


Top 5 Nutritional Ketosis Mistakes—And How to Fix Them




Key Takeaways
- A well-formulated ketogenic diet keeps protein moderate and uses fat as the main energy source, with adequate dietary fat needed for satiety and ketone production.
- The best keto fats are mostly monounsaturated and saturated fats, while concentrated vegetable oils, trans fats, and excess omega-6 fats should be limited.
- Adequate sodium is essential on a ketogenic diet, and many people need about 5 grams of sodium per day to avoid fatigue, dizziness, headache, and constipation.
- Virta Health provides individualized ketogenic support that helps people set the right protein, fat, carbohydrate, and sodium targets while safely managing blood sugar, weight, and medication changes.
Having trouble getting your ketones up, dealing with side effects, figuring out your protein intake, and/or finding the right fats? We’re here to help.
Problems we'll help you avoid:
- Low blood ketones
- Stomach upset and fat intolerance
- ‘Keto flu’ (fatigue, dizziness, headache, constipation)
- Getting misled by arbitrary ‘macros’ rather than individualized intake goals
- The metabolic rollercoaster with some versions of fasting
Nutritional ketosis is a powerful metabolic state in which your body primarily burns fat and ketones rather than glucose for fuel, which occurs when dietary carbohydrate intake is reduced (not eliminated) below your personal threshold of carbohydrate tolerance. Once ketosis is achieved and maintained, the metabolic benefits are bountiful: safe and effective weight loss (Sachner-Bernstein 2015), reduced hunger and cravings (Boden 2005), decreased inflammation (Forsythe 2008), lower and more stable blood sugar (thus, reversal of Type 2 diabetes) (McKenzie 2017; Hallberg 2018), and beyond.
The length of time it takes a person to adapt to nutritional ketosis varies from one individual to the next, as each person has a unique biochemistry and varying degrees of metabolic damage needing repair. With very rare exceptions (Corti 2008), it is possible for everyone to enter nutritional ketosis. In fact, all of us are exposed to nutritional ketosis as newborn infants if we are exclusively breastfed (Cahill 2006). So, if weeks or even months have passed and you are still struggling, you may be falling prey to one of these common mistakes that can interfere with nutritional ketosis.
Dr. Stephen Phinney on the Top 5 Ketosis Mistakes
Mistake #1: Too much protein, not enough fat
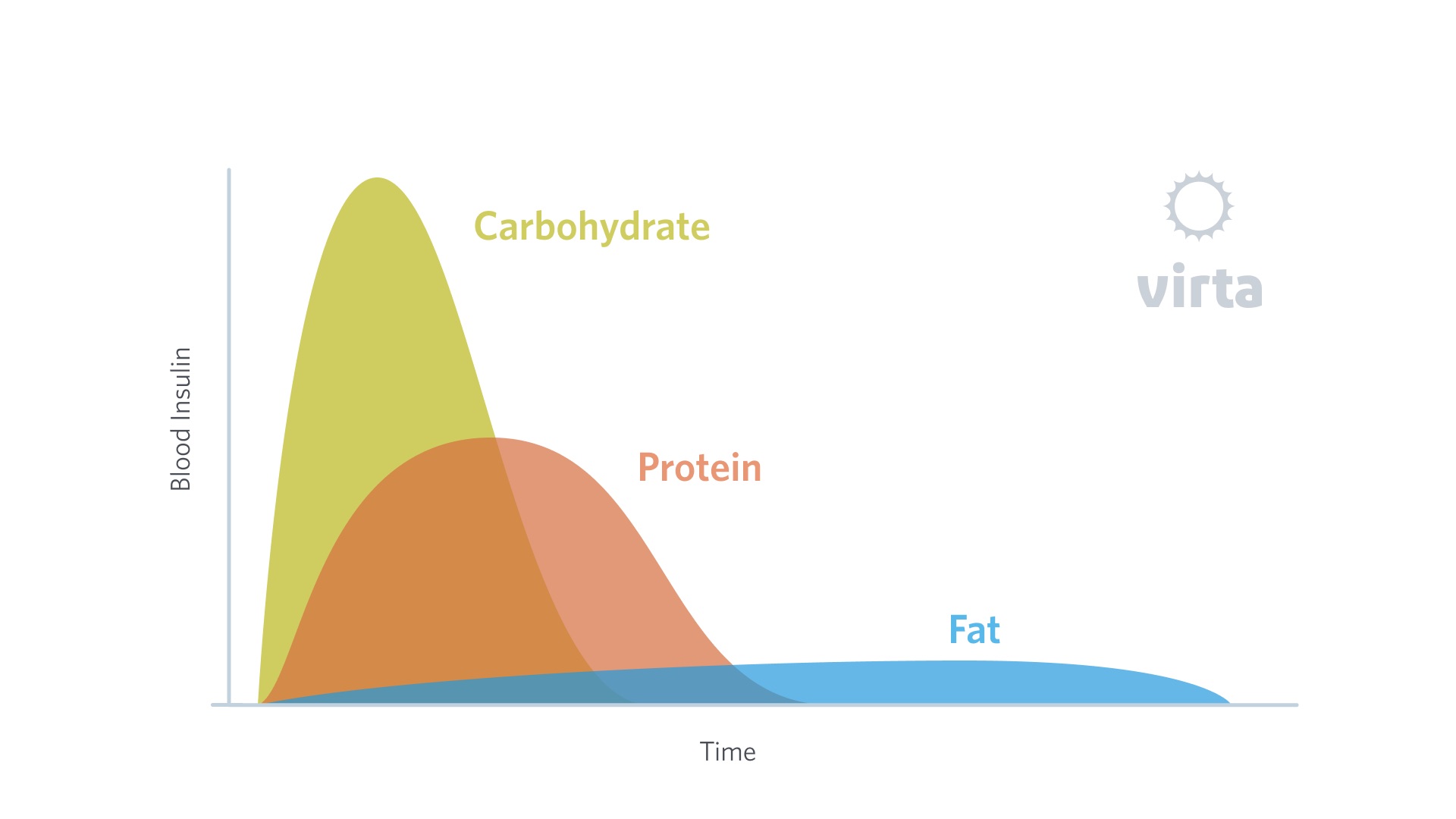
A well-formulated ketogenic diet is moderate, NOT HIGH, in protein. Protein has a moderate insulin-stimulating effect, and although it’s less than the impact from a similar amount of carbohydrates, it can interfere with ketone production by the liver when consumed in excess. Most healthy individuals require between 1.5 and 1.75 grams of protein per kg of ‘reference body weight’ (Phinney 1983, Davis 1990) to maintain lean body mass and function during a ketogenic diet. Intakes above 2.0 g/kg reference weight show no additional benefit. Here's where you can find your protein needs on a ketogenic diet.
It is common for people consuming a ketogenic diet to think they are consuming protein in moderation when they are actually well above this in reality. When hunger strikes, it’s just easy to grab a protein source for a fix -- nuts and cheese are among the most satisfying low carbohydrate snacks, especially if your dietary fat intake is inadequate. Calories from FAT should make up the majority of your dietary intake in order to feel adequately satisfied. While dietary fat is typically associated with protein-rich foods (like those nuts and cheeses, as well as eggs and meats), ultimately, even the fattiest protein sources will fail to provide satiety while staying within your recommended personal protein goal. Adding fats like olive oil, butter, cream, coconut, or canola oils to meals without being accompanied by extra protein is critical to achieve both satiety and nutritional ketosis. If you remain fearful of adding dietary fat to your meals, now is the time to critically re-evaluate those fears.
Mistake #2: Choosing the wrong kinds of fat
When it comes to consuming dietary fat, it’s not only about quantity, but quality, too.
Fat is essential and two of its primary functions in humans are: 1) as a fuel source, particularly when “keto-adapted,” and 2) to build and maintain vital membranes for all the cells in the body.On a ketogenic diet, monounsaturated and saturated fats should provide the majority of your dietary fat intake to supply the body with energy, as the body prefers to use these types of fats for fuel.
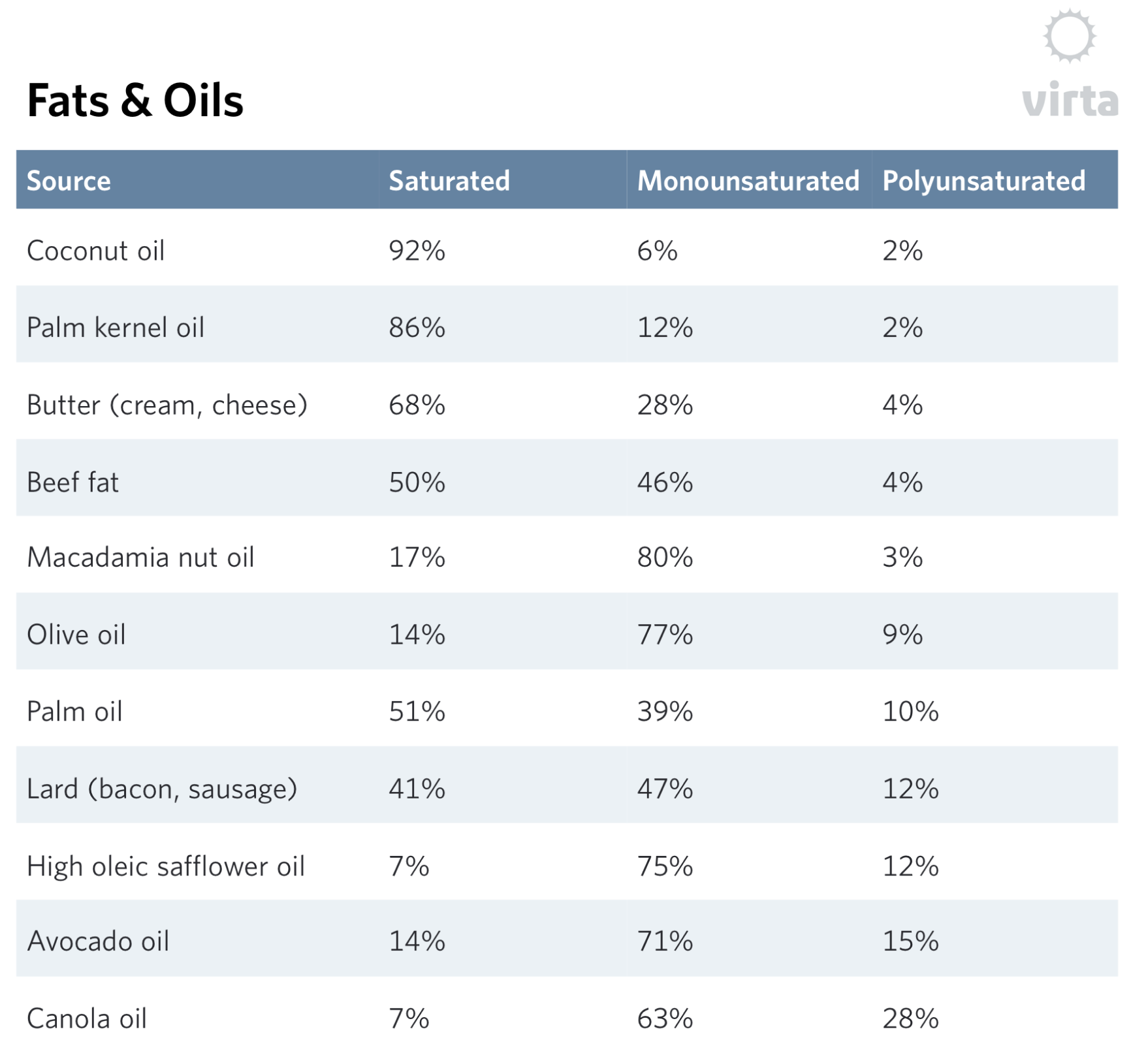
Monounsaturated and saturated fat sources are both readily available and delicious. Monounsaturated fats are found in abundance in certain oils such as olive, avocado, and canola, as well as in some animal fats such as lard. Saturated fats are naturally concentrated in most animal fats such as dairy fat, beef (suet), and lamb, as well as “tropical oils” (e.g., coconut and palm oil). Dietary saturated fats are readily burned off to be used for fuel (i.e., they won’t accumulate in your blood) when a person is keto-adapted.
Polyunsaturated fats, on the other hand, are only required in small quantities and are not well-tolerated in large amounts. Therefore, highly concentrated sources such as most vegetable oils should be limited and avoided whenever possible. Common sources of polyunsaturated fat include soybean, corn, sunflower, safflower, cottonseed, and peanut oils. Note, however, that high monounsaturated versions (also called ‘high oleic’) of safflower, sunflower and even soybean oils are coming into the market; and this will make avoiding excess omega-6 fats both easier and more economical.
That being said, two sub-classes of polyunsaturated fats, omega-6 and omega-3, are essential to consume in small amounts for the purposes of membrane health, as our bodies cannot naturally make them. To consume the recommended amount of omega-3 fatty acid, eat 3 servings of cold-water ocean fish per week (even canned tuna is OK) or take at least 1 gram of fish oil daily (or flaxseed oil if you are vegetarian or vegan). In contrast, the absolute requirement for omega-6 is minor compared to what the average American eats, so even on a low fat diet it would be quite hard not to get enough. Consuming excess omega-6 fats, however, will lead to stomach and intestinal upset and possibly increase inflammation.
Finally, avoid artificial trans fats all together, such as commercial shortening and margarine, as they are strongly linked to coronary artery disease (Mozaffarian 2006).
The “right” fats to choose are outlined below.
Mistake #3: Not enough salt
After decades of the media propagating low sodium diets, do you find yourself actively avoiding salt? If so, you may be susceptible to the common pitfall of not consuming enough of this critical mineral, putting you at risk for some pesky side effects.
Current US dietary guidelines recommend 2300 mg of sodium per day. However, recent research published in mainstream journals like the New England Journal of Medicine highlights that consuming 2300 mg or less of sodium daily actually increases mortality in the general healthy adult population; in fact, for optimal health, most of us need anywhere between 4000-5000 mg of sodium per day -- and that’s for people consuming standard diets containing appreciable amounts of carbohydrate (O’Donnell, 2014).
On a ketogenic diet, consuming adequate sodium becomes all the more critical, as the rate of sodium excretion by the kidneys into the urine increases quite significantly while in nutritional ketosis. This means that most people on a ketogenic diet need to consume closer to 5000 mg (i.e., 5 grams) of sodium -- which equals 12 grams of salt -- per day in order to maintain an adequate balance. Starting in just the first few days of adapting to nutritional ketosis, neglecting to consume 5 grams of sodium can put your circulatory system into disarray and trigger the notorious “keto flu” symptoms: headaches, dizziness, lightheadedness, fatigue and constipation. And here’s an important point: this daily need for 5 grams of sodium continues as long as one remains in nutritional ketosis; it’s not just a temporary need during keto-adaptation as some bloggers would have you believe.
Fortunately, you can keep these symptoms at bay and improve your overall well-being and function by simply salting your food moderately and consuming 2 servings of broth or bouillon daily. For most people, this results in about 3 grams of sodium from regular food plus 2 grams from broth, totaling 5 grams per day. Keep in mind that salt and sodium are not the same —1 teaspoon of salt is the equivalent of 5 grams of salt but contains only 2.3 grams of sodium (the rest is chloride).
Note: please consult a medical professional if you have high blood pressure or fluid retention due to congestive heart failure or kidney problems to determine the right dietary sodium intake for you.
Mistake #4: Stagnant "macro ratios”
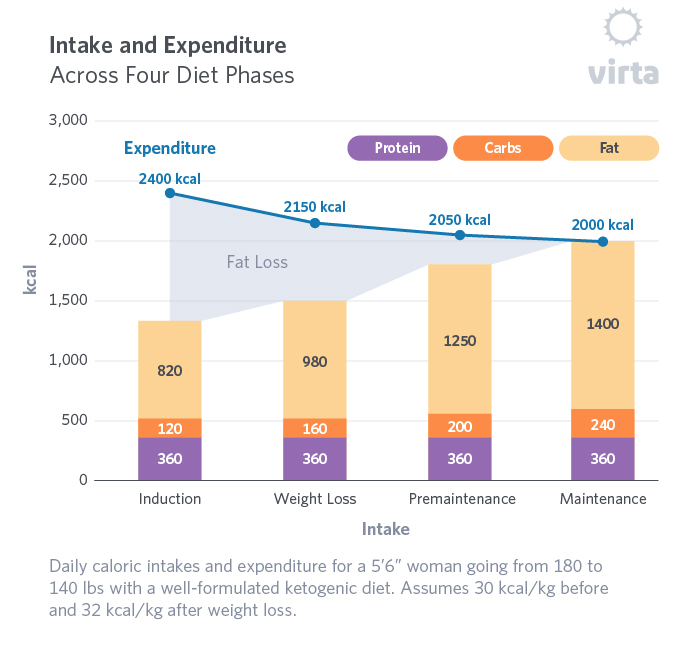
There are three major macronutrients (or “macros”) that supply humans with energy (calories) from foods: carbohydrate, fat, and protein. On a well-formulated ketogenic diet, your daily energy needs should be satisfied by approximately 5-10% carbs, 70-80% fat, and 15-20% protein.What people frequently overlook is the fact that when you initially begin a ketogenic diet and are losing weight, a significant portion of that 70-80% of energy from fat will actually come from burning your own body fat stores from adipose tissue—so it’s NOT entirely from dietary sources. Later down the road as you approach “weight maintenance” and are aiming to remain weight-stable while keeping your energy levels high and metabolic health at optimum, the fat needed to supply your daily energy will have to come from your food. After all, in this scenario you no longer have as much excess fat to lose! The chart below shows food macronutrient intakes plus body fat contributions as one progresses from through the stages of weight loss to eventual weight stability.
Although your intake of dietary fat will need to increase, no matter if it’s Day 1 or Day 500, you will continue consuming approximately the same, moderate amount of protein in addition to non-starchy vegetables (your main source of carbohydrates plus essential vitamins and minerals). Depending on your personal health goals, and particularly how well your initial diabetes or prediabetes is held in reversal, some people may be able to increase their carbohydrate intake somewhat in maintenance.
So while it seems counterintuitive for someone wanting to stay slim, you will need to eat more fat as you approach and then achieve weight maintenance. This means that you can give yourself permission to increase your consumption of the tasty, “right” types of fats discussed above, which will become a cornerstone of your success.
Dr. Phinney on macros
Mistake #5: “Needing” to fast
You may have noticed a recent frenzy of people advocating fasting as potent tool for rapid weight loss, enhancing ketone levels and increasing life span. But think twice before deliberately enduring calorie-free days. Much of the research supporting these benefits has been done in mice. Well-done human research on the long-term safety and efficacy of fasting raises important concerns, particularly if one chooses to fast longer than one day. Fasting for more than 2 days can lead to lean tissue loss and even a permanent reduction in reduction resting metabolism (Fothergill, 2016), among other significant health concerns.
Of particular concern to us is when periods of fasting, whether short or long, are performed by people taking medication for diabetes or high blood pressure. Going in and out of the fasting state while on these medications can lead to dangerous swings in blood glucose or blood pressure, and this is risky if done without close, expert medical supervision.
In contrast, achieving and maintaining a stable state of nutritional ketosis with real food while avoiding majorly wide swings in your daily caloric intake and medication needs will be not only safer and more sustainable, but more enjoyable to boot.
This blog is intended for informational purposes only and is not meant to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or any advice relating to your health. View full disclaimer
Are you living with type 2 diabetes, prediabetes, or unwanted weight?

Boden, G; Sargrad K, Homko C, Mozzoli M, Stein TP. Effect of a Low-Carbohydrate Diet on Appetite, Blood Glucose Levels, and Insulin Resistance in Obese Patients with Type 2 Diabetes. Ann Int Med. 2005
Corti S, Bordoni A, Ronchi D, et al. (March 2008). "Clinical features and new molecular findings in Carnitine Palmitoyltransferase II (CPT II) deficiency". Journal of the Neurological Sciences. 266 (1–2): 97–103. doi:10.1016/j.jns.2007.09.015. PMID 17936304
Cahill GF Jr. Fuel Metabolism in Starvation. Annu. Rev. Nutr. 2006; 26:1–22 doi: 10.1146/annurev.nutr.26.061505.111258
Davis PG, Phinney SD. Differential effects of two very low calorie diets on aerobic and anaerobic performance. Int J Obes. 1990 Sep;14(9):779-87
Forsythe CE, Phinney SD, Fernandez ML, Quann EE, Wood RJ, Bibus DM, Kraemer WJ, Feinman RD, Volek JS. Comparison of low fat and low carbohydrate diets on circulating fatty acid composition and markers of inflammation. Lipids. 2008; 43:65-77.
Fothergill, E., Guo, J., Howard, L., Kerns, J. C., Knuth, N. D., Brychta, R., Chen, K. Y., Skarulis, M. C., Walter, M., Walter, P. J. and Hall, K. D. (2016), Persistent metabolic adaptation 6 years after “The Biggest Loser” competition. Obesity, 24: 1612–1619. doi:10.1002/oby.21538
Hallberg SJ, McKenzie AL, Williams P, et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at One Year: An Open Label, Non-Randomized, Controlled Study. Diabetes Ther. 2018. DOI: 10.1007/s13300-018-0373-9
McKenzie A, Hallberg S, Creighton BC, Volk BM, Link T, Abner M, et al. A Novel Intervention Including Individualized Nutritional Recommendations Reduces Hemoglobin A1c Level, Medication Use, and Weight in Type 2 Diabetes. JMIR Diabetes. 2017;2(1):e5
Mozaffarian D, Katan ME, Ascherio A, Stampfer MJ, Willett WC. Trans fatty acids and cardiovascular disease. N Engl J Med 2006;354: 1601-13
O’Donnell M, et al. N Engl J Med 2014; 371:612-623. 102,000 people assessed for urinary sodium and then followed for 3.7 yrs
Phinney SD, et al. The human metabolic response to chronic ketosis without caloric restriction: physical and biochemical adaptation. Metabolism. 1983; 32:757-768
Sackner-Bernstein J, Kanter D, Kaul S. Dietary Intervention for Overweight and Obese Adults: Comparison of Low-Carbohydrate and Low-Fat Diets. A Meta-Analysis. PLoS One. 2015; https://doi.org/10.1371/journal.pone.0139817





